Why does my resting heart rate go up after AF ablation?

In the era of wearables and heart rate trackers, this phenomenon is being picked up incidentally by patients in the weeks or months after successful catheter ablation for their Atrial Fibrillation. So before you let anyone convince you that you’re just being paranoid, read on…

How high is too high?
A high heart rate can mean different things and if you suspect an abnormality or change in heart rhythm or rate after your ablation, the first step should be getting an ECG. Atrial Fibrillation, Atrial Tachycardia or Atrial Flutter can potentially come on after ablation and so the ECG will help rule this out.
The rest of this article will focus on a high heart rate during sinus rhythm. And high does not mean over 100 beats per minute, it simply means higher than the resting sinus rhythm heart rate before the ablation. For example, if your resting heart rate or night-time heart rate was always 60-70 beats per minute and now your Fitbit/Watch/blood pressure machine is showing 70-80 beats per minute when you're at rest, this may be disconcerting. Especially for patients with AF who have been in the habit of associating increased heart rate = AF. However, the physiology behind this suggests it may be the opposite and could be a good sign.
Why does the heart rate increase?
It is due to the nerves that supply the heart. If you isolate a heart but retain its blood supply, it will beat at its internal rate of the sinus node which is 100 beats per minute.
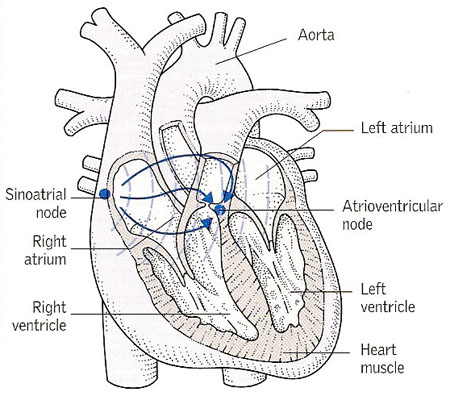
The heart has a rich supply of nerves originating from the body’s “fight or flight” system. Branches of the vagus nerve supply the heart and suppress the internal heart rate. That is why a resting heart rate usually sits at 50-90 beats per minute- not 100bpm.
Several smaller branches of the vagus nerve connect to the outside surface of the left atrium of the heart. Catheter ablation applies treatment to wall of the left atrium to render sections electrically inactive- blocking the AF from entering and taking over. Good ablation treats the whole wall thickness as the AF electrical impulses can flow through the inner or outer surface of heart. If a treated area sits beneath one of these vagal branch connections, it will reduce the amount it suppresses the internal heart rate and so the heart rate will rise.
These vagal branches connect in different positions in different people. That’s why some patients may experience this phenomenon and others may not.
Am I at higher risk of AF coming back?
We see the opposite! As said, ablation is most effective if it treats the full thickness of the heart muscle and so if the vagal branches are reached, that means the ablation there was full thickness.
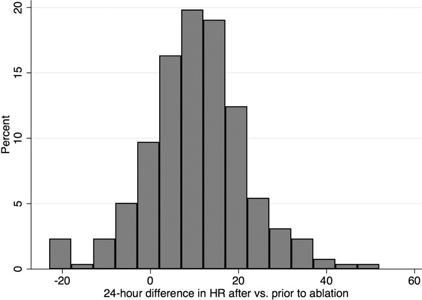
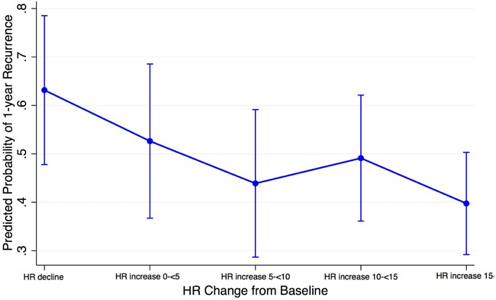
The Johns Hopkins Hospital AF group studied the rate of AF recurrence in patients after AF ablation, comparing patients based on their change in heart rate after ablation. They found an inverse relationship- meaning the higher the heart rate, the lower the chance of AF recurrence. In patients that had an increase of 15beats (i.e. from 50bpm to 65bpm or 75bpm to 90bpm) after ablation, their risk of AF recurrence was less than half that of patients who had a heart rate decrease.
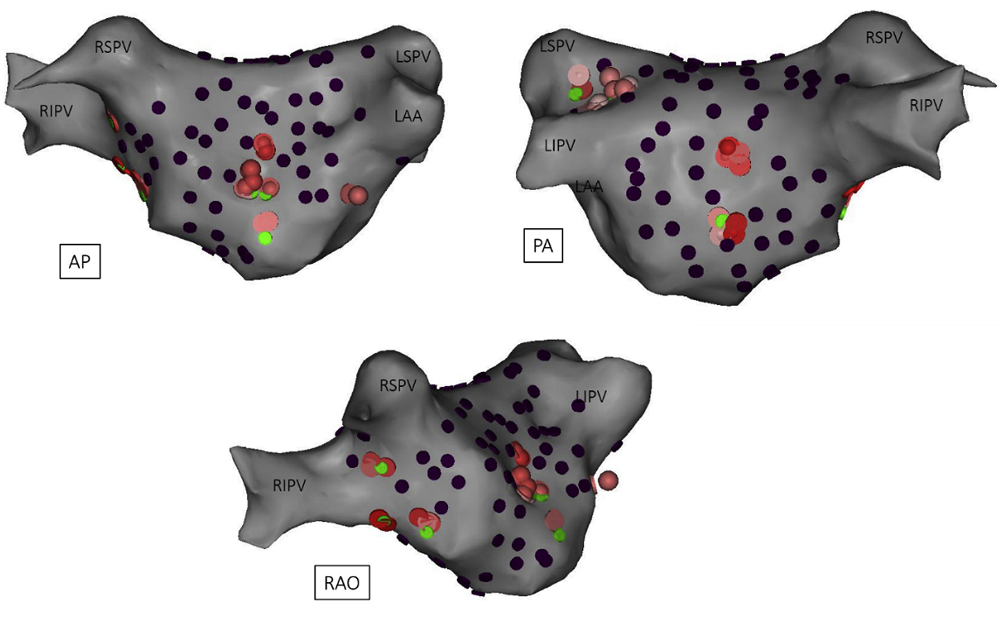
On this basis, Research Groups from Russia and the UK have even tried to target these regions during the ablation procedure to see if it will improve outcomes. This approach hasn’t clearly shown benefit yet- but this may partly be because of the challenges of identifying the vagal nerve connection sites and treating them.
Should I take medications for this?
So in the absence of any evidence of health risk of AF recurrence risk, there is no role for rate control medications in sinus rhythm. This phenomenon can also resolve by itself after a year or so and the heart rate adjusts back down to its original resting rate.
But note- medication may also be a reason for a change in resting heart rate. If you were taking a tablet to suppress your AF episodes- like bisoprolol, sotalol or diltiazem these may also have been suppressing your heart rate pre-ablation when in normal sinus rhythm. So if you have now stopped that after successful ablation- you may notice your resting heart rate rise after coming off the medicine. Again this is not concerning and in itself not a reason to continue taking a tablet.
The sensation of “extra” heartbeats or “missed” beats after ablation is another story that will be covered next week.
The Johns Hopkins paper: Goff ZD, Laczay B, Yenokyan G, Sivasambu B, Sinha SK, Marine JE, Ashikaga H, Berger RD, Akhtar T, Spragg DD, Calkins H. Heart rate increase after pulmonary vein isolation predicts freedom from atrial fibrillation at 1 year. J Cardiovasc Electrophysiol. 2019 Dec;30(12):2818-2822. doi: 10.1111/jce.14257. Epub 2019 Nov 10. PMID: 31670430.
The Imperial College London paper: Kim MY, Coyle C, Tomlinson DR, Sikkel MB, Sohaib A, Luther V, Leong KM, Malcolme-Lawes L, Low B, Sandler B, Lim E, Todd M, Fudge M, Wright IJ, Koa-Wing M, Ng FS, Qureshi NA, Whinnett ZI, Peters NS, Newcomb D, Wood C, Dhillon G, Hunter RJ, Lim PB, Linton NWF, Kanagaratnam P. Ectopy-triggering ganglionated plexuses ablation to prevent atrial fibrillation: GANGLIA-AF study. Heart Rhythm. 2022 Apr;19(4):516-524. doi: 10.1016/j.hrthm.2021.12.010. Epub 2021 Dec 13. PMID: 34915187; PMCID: PMC8976158.