Valvular AF


Do I have valvular AF?
If you were born in the UK and have AF, the probability is low. However, if you were born in India or Africa, the chances are much higher! Read on...
When AF co-exists with a condition called "rheumatic heart disease" (an autoimmune reaction to throat infections that damages heart valves) it is known as 'valvular AF'.
Although 40 MILLION people worldwide have rheumatic heart disease, it's become increasingly rare in the Western world with improved antibiotic treatments but it can often occur during childhood and the valve damage only detected later on when you have another linked heart condition like AF.
That's why your Cardiologist will always do an echo scan of the heart and valves if you have AF.
But why's this important?
Putting the valve damage to one side, it has consequences for how your AF is managed too. That's because valvular AF is thought to carry a higher stroke risk and so whilst patients with 'non-valvular AF' (the MUCH more common version in the UK) have been transitioned onto the new generation of anticoagulants (like apixaban, edoxaban, rivaroxaban, dabigatran), patients with valvular AF have not- they have been told to remain on warfarin.
So why are we discussing this today?
Last weekend was the 'European Society of Cardiology Congress 2022'- the largest Cardiology conference in the World and a lot of exciting research was published, including the INVICTUS trial- the first randomised controlled study on which anticoagulant was better in valvular AF- warfarin vs the new generation drugs? The new generation drugs have a clear benefit in the communities where valvular AF is most prevalent- regular blood tests for warfarin dosing is HARD to access and so a 'one-stop and go' new generation drug would be helpful.
The study recruited 4565 patients from 24 different countries 🤯 and randomised half to Warfarin and half to the Rivaroxaban (note: the study was sponsored by the manufacturer of this new generation anticoagulant).
To set the scene a little, these large-scale, multi-centre, randomised controlled studies have shown benefit of the new generation of drugs in non-valvular AF a number of times over and that's what led to the International guidelines recommending them in preference to warfarin.
However, in INVICTUS, the opposite was seen. Amongst patients with AF and rheumatic heart disease, the survival results (from strokes, heart attacks, blood clots, blood vessel problems) over 3 years favoured warfarin use. There was no significant difference in bleeding events either (something that has been higher in warfarinised patients during the non-valvular AF studies).
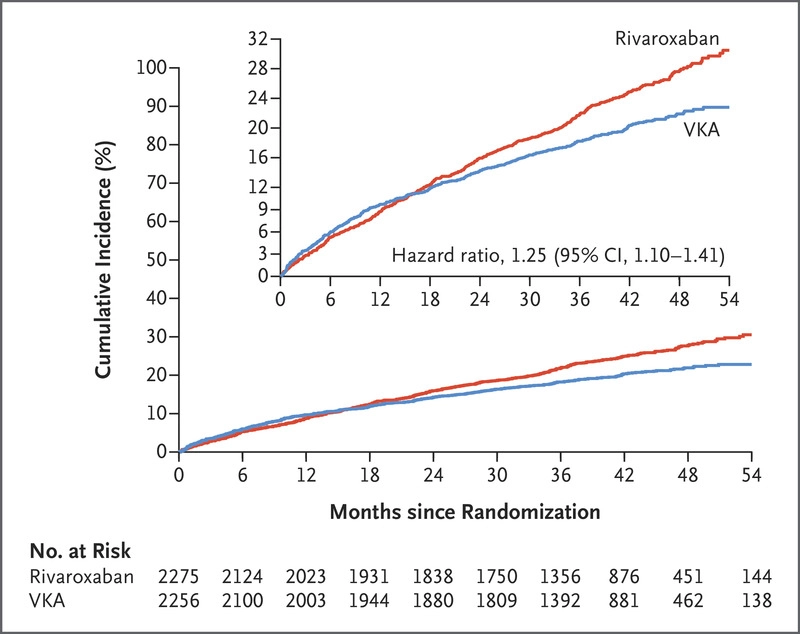
So, in summary, we now have quality evidence to support the status quo for valvular AF patients, warfarin should remain the standard of care in this group of patients. Other niche patient groups that may benefit from warfarin over the new drugs include patients with mechanical valve replacements- but ultimately this has to be an individualised decision between each patient and their physician.
Full paper below:
Connolly SJ, Karthikeyan G, Ntsekhe M, Haileamlak A, El Sayed A, El Ghamrawy A, Damasceno A, Avezum A, Dans AML, Gitura B, Hu D, Kamanzi ER, Maklady F, Fana G, Gonzalez-Hermosillo JA, Musuku J, Kazmi K, Zühlke L, Gondwe L, Ma C, Paniagua M, Ogah OS, Molefe-Baikai OJ, Lwabi P, Chillo P, Sharma SK, Cabral TTJ, Tarhuni WM, Benz A, van Eikels M, Krol A, Pattath D, Balasubramanian K, Rangarajan S, Ramasundarahettige C, Mayosi B, Yusuf S; INVICTUS Investigators. Rivaroxaban in Rheumatic Heart Disease-Associated Atrial Fibrillation. N Engl J Med. 2022 Aug 28. doi: 10.1056/NEJMoa2209051. Epub ahead of print. PMID: 36036525.