'Pace and Ablate' part 1


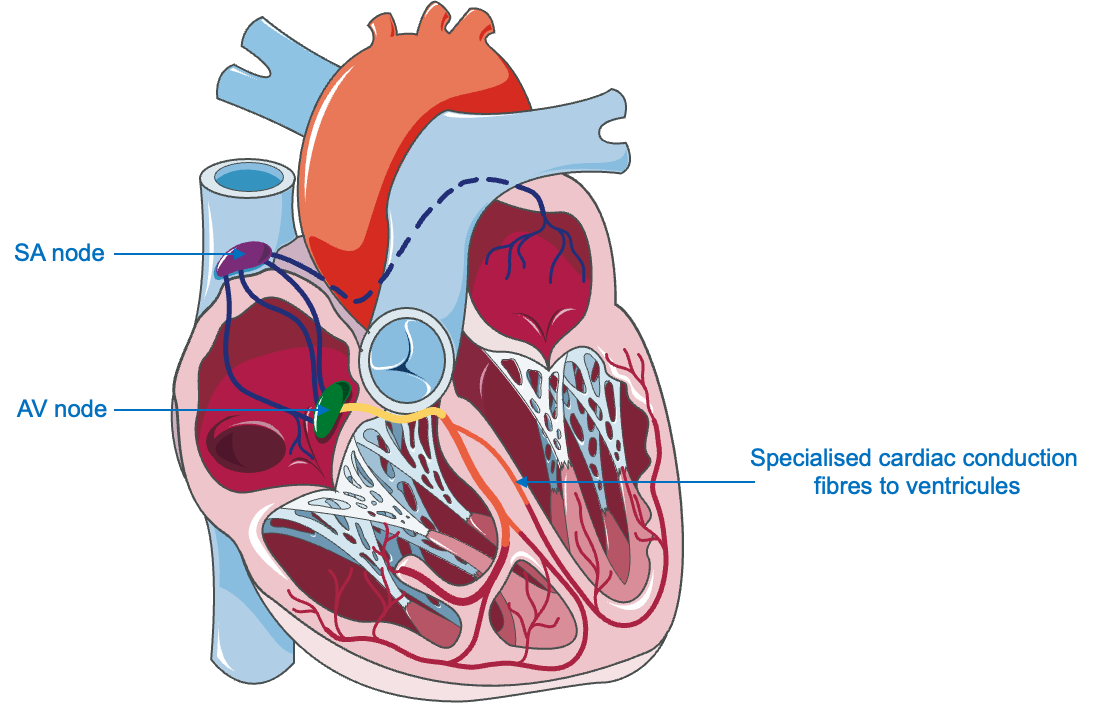
'Pace and ablate' is short-hand for 'implant a pacemaker and perform an AV node ablation'. It is a treatment for atrial fibrillation because the 'AV node ablation' part blocks any intrinsic heart rhythm from setting the heartbeat and the implanted pacemaker takes over, ensuring the heart rhythm always stays steady and controlled. This latter component; the irreversible replacement of heart rhythm conduction can be of value if the underlying rhythm is fast, uncontrollable AF causing symptoms but it is a major commitment and so it is rarely performed as a first-line treatment.
However, it is technically very effective. Whereas AF can come back after medicines or ablation procedures, There is no way it can if you knock out the AV node (but there's no chance of restoring natural heart rhythm either). It's a major undertaking- but is there benefit?
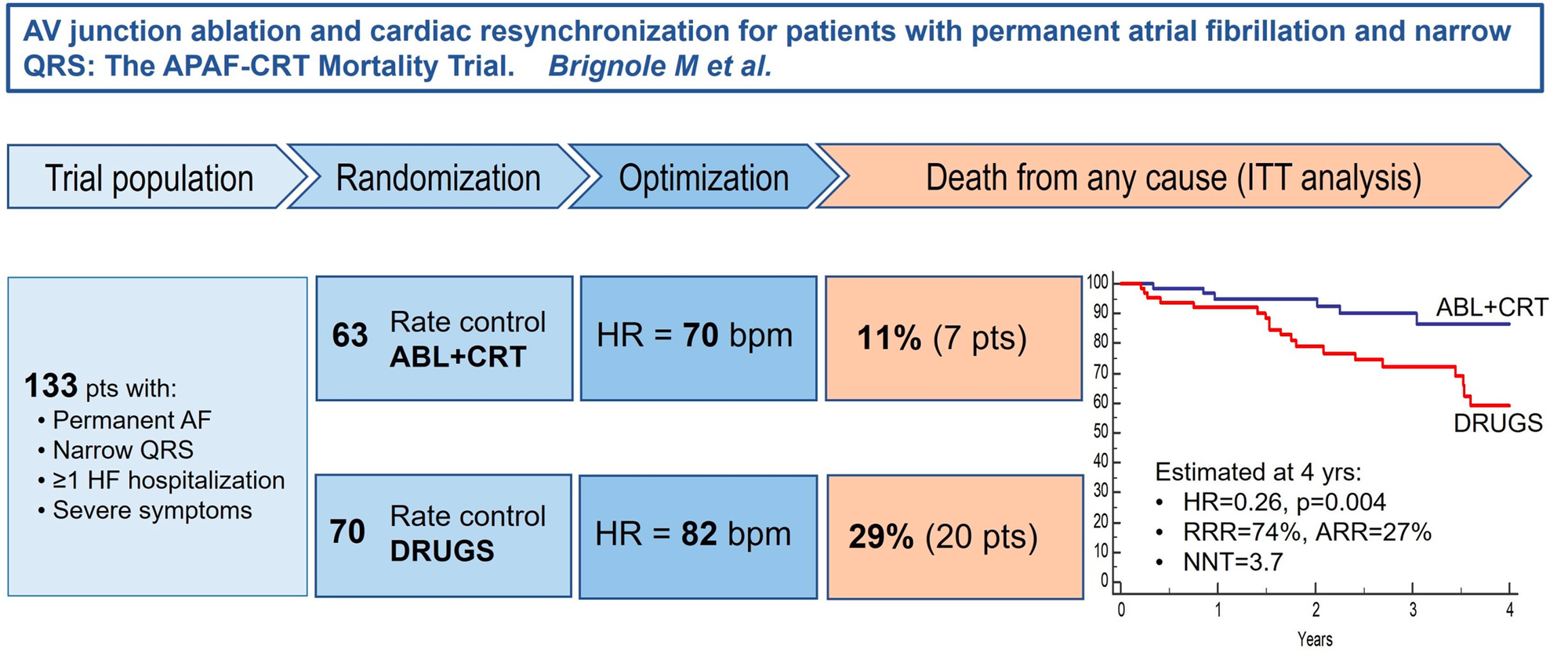
The APAF-CRT trial compared 'pace and ablate' in patients with permanent AF and heart failure against rate control medicines. They enrolled 133 patients and used a special type of pacemaker called a CRT for the 'pace and ablate' arm and followed them up for 2 years to measure the impact on survival.
The APAF-CRT trial results were published in 2021. The investigators found a 74% reduction in death with 'pace and ablate'. This was a relatively small study of a very specific group of AF patients- but a 74% reduction in death is remarkable for a non-emergency treatment procedure. I can't think of a contemporary elective treatment in Cardiology that has demonstrated such a dramatic treatment benefit (I'll keep looking but this is greater than stents for stable angina or defibrillators for heart failure). Again, let me stress this is one small study in a specific AF sub-group and we should not get carried away, but it's certainly worth investigating further.
Remember- the patients enrolled in the research study were highly selected. The APAF-CRT investigators excluded patients with a 'bundle branch block' (another ECG abnormality) or with only 'mild' heart failure symptoms. The average age was >70 years old and these patients were all deemed unsuitable for AF ablation or had failed it already. These were the sickest AF/HF patients poorly controlled rates with severe symptoms despite many medications.
So extrapolating these results to any patient with AF is inappropriate. AV node ablation is an irreversible procedure that leaves the patient entirely dependent on the pacemaker for their heartbeat. The human heartbeat is a complex process that responds to exercise, that slows in sleep, and causes the different chambers of the heart to beat in synchrony. Pacemakers are becoming increasingly advanced but they cannot replace all the functionality of our natural heartbeat and so it is not a step to take lightly. It isn't a first-line treatment currently and so it was reasonable for this study to evaluate it in the sickest patients who may have tried and failed other treatments.
But still, this result is a significant step forward, in that selected patients who have tried medicines, tried ablation, and still have symptomatic AF may have a final option that can improve their symptoms, reduce their risk of hospitalisation and reduce their mortality!
'Pace and ablate' absolutely eliminates the heart rhythm irregularity of AF- whether this is the feature that drives part of the benefit seen here is something we're investigating in the AFHF study. So thank you to all the patients generously participating in this Trial! 🙏
Next week, we'll review the PABA-CHF study; that compared 'pace and ablation' with AF catheter ablation in patients with heart failure. Stay tuned! 🎹