Does an AFib ablation make you live longer?

Several trials have explored this- but do we have enough evidence to say yes?
People with AF have an increased risk of death
Atrial Fibrillation is a chronic disease. Patients live with it in the same way patients live with Diabetes or Coronary Disease. But do people who develop AF die earlier?Large observational studies such as the Framingham Heart Study (a long-term population-based study since 1948 of more than 5000 individuals living in Framingham) have been able to report on this. The residents with AF unfortunately had a higher rate of death during the follow-up period than people without AF. This was after balancing for other potential differences that may effect survival such as diabetes, smoking, age- the risk was 1.5x greater in people with AF than in matched group of people without AF.
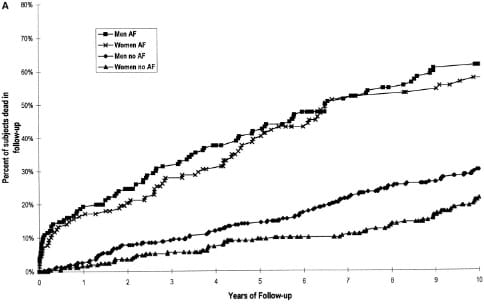
We know that patients with AF have a higher risk of stroke (hence why blood thinners are the first pillar of care), heart failure and sudden death than patients without AF that contribute to this difference.
But as doctors, a crucial question we have to ask is- if we can suppress the AF- do people live longer? This is especially important in the context of AF Ablation- the treatment is not completely risk-free so, we need to know the extent of benefit we can tell a patient they may receive to justify them taking these risks. If there is a survival benefit, then perhaps there are reasons to think about Catheter Ablation even if someone is asymptomatic.
Does Catheter Ablation of AF reverse the risk?
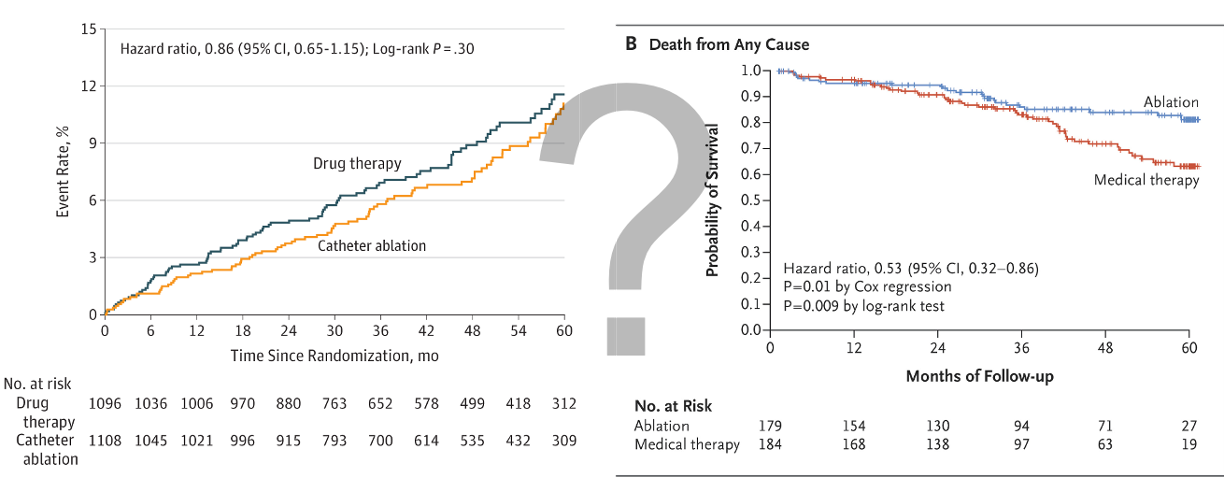
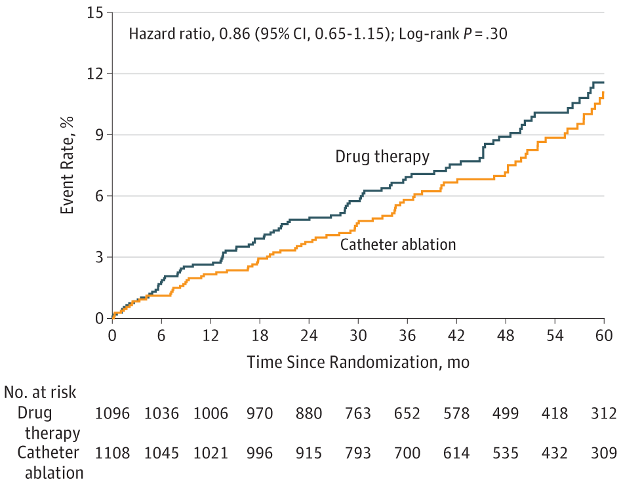
Several studies have shown that patients who have Catheter Ablation of their do live longer than patients who do not. But this does not mean Catheter Ablation causes these patients to live longer. Patients who are referred for ablation are usually healthier, younger and have fewer medical issues than patients who are not. Combining lots of these studies suggested there may be a survival benefit and so that is why the American National Institute for Health funded the CABANA trial. 2204 patients with symptomatic AF from 126 centres (including Barts) were enrolled and randomised to either receive AF catheter ablation or medical treatment only.
When the results were announced at the Heart Rhythm Society Conference in 2018, there was an audible gasp in the audience- no significant difference between the two groups in terms of the rate of death, stroke, bleeding or cardiac arrest. The rates of death were similar (5.2% vs 6.1% over approximately 4 years). Without going too deep into the controversy, there were a lot of comments that many patients in the medicine group (27.5%) were actually treated with ablation so may have diluted the benefit. So this may be something that is may one day be re-visited.
But the bottom line is that in the 'general' patient undergoing AF ablation for symptom improvement- we do not have strong evidence that it will make people live longer.
But if you have Heart Failure- it may be different
Last week I covered the change in the American AF guidelines- upgrading their recommendation for AF catheter ablation in selected Heart Failure patients to class 1a (the highest recommendation level they can issue). This was because of the evidence showing AF Ablation in patients with Heart Failure and pump weakness feel better, are able to exercise more, stay out of hospital longer and improve their heart function on echo scans.
But their primary driver for the upgrade was their consideration of two trials evaluating survival benefits after AF ablation in Heart Failure. But the evidence isn't black and white.
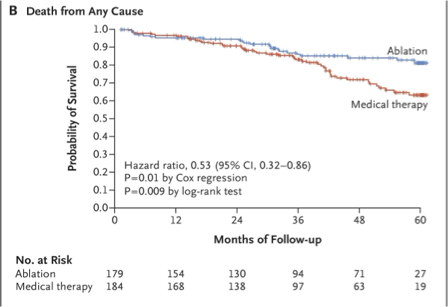
Trial 1: CASTLE-HF
The CASTLE-HF trial is the most commonly referenced paper when the survival beenfit of Catheter Ablation of Heart Failure patients is discussed. The investigators, enrolled 363 patients with symptomatic AF and heart failure. They selected patients with Heart Failure with severe pump weakness (their ejection fraction on echo scan was less than 35%) and they were followed up for 5 years. The rate of death in the catheter ablation group of patients was almost half (24 out of 179 [13.4%] vs. 46 out of 184 [25.0%]). The rate of Heart Failure hospitalisation was lower too. However, this trial has not been without criticisms- Reviewers draw attention to the atypical group of heart failure patients that were enrolled (it took them 8 years to enrol 363 patients after considering 3013 patients) so the findings may not apply to all heart failure patients. Some patients were 'lost to follow-up' (a Research term for could not be contacted during follow-up and so excluded from the final dataset. This loss of data may introduce bias and weaken the findings. Nevertheless, it was a big difference in outcome and probably a key factor in the class 1a recommendation.
Trial 2: RAFT-AF
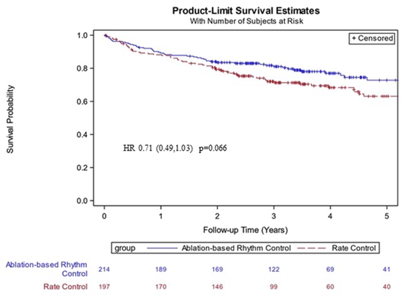
The "Randomized Ablation-Based Rhythm-Control Versus Rate-Control Trial in Patients With Heart Failure and Atrial Fibrillation" was a second study of the survival benefit of Catheter Ablation in Heart Failure. An important difference from the patients enrolled in CASTLE-HF was that the investigators randomised 411 patients with AF and either type of Heart Failure (so not just patients with pump weakness, but any patient with Heart Failure symptoms and abnormal Heart Failure-related blood tests.)
In terms of their results- The first line of the abstract conclusion was:
In patients with high-burden AF and HF, there was no statistical difference in all-cause mortality or HF events with ablation-based rhythm control versus rate control.
which they followed up with...
...however, there was a nonsignificant trend for improved outcomes with ablation-based rhythm control over rate control.
From a statistical point of view, the difference in survival between patients undergoing ablation versus those randomised to medical treatment only was not significant i.e. may have been caused by random chance. The difference was so apparent that the trial was terminated early because of apparent futility.
What if we combine all the survival data?
This is what the American guideline writers considered. It's a technique in medical research called meta-analysis- a statistical technique that combines the results of multiple scientific studies to provide a more comprehensive understanding of a particular topic or question. In this case, CASTLE-HF and RAFT-AF and any other studies that looked at this question as a secondary objective were combined.
For example, in the CABANA study (the one discussed at the top that showed no survival benefit in the general AF population), 778 of the patients enrolled in the study had Heart Failure. A sub-analysis of just this group alone showed improvement in survival compared with the medical therapy group. The same in the EAST-AFNET trial that we discussed earlier in the year. When you combine the results- catheter ablation for AF was associated with significant benefits in all-cause mortality and the frequency of Heart Failure hospitalisation.
The definitive trial is coming
And a definitive trial to give us a final answer to this question is about to get underway. The CRAAFT-AF trial has been approved and funded in the UK and is set to be the largest trial of AF Catheter Ablation in Heart Failure patients. Prof Pier Lambiase, the Study Principal Investigator and Consultant here at Barts is looking to enrol 1200 patients from sites across the Country and Europe. The study will randomise Heart Failure patients to receive AF ablation or medical treatments only. It will compare the rates of survival in the two groups over a 4-year period.
It will enrol patients both types of Heart Failure (with or without pump weakness). We hope to enrol our first patients from Barts Hospital early next year.