The Atrial Fibrillation trials that will change 2024


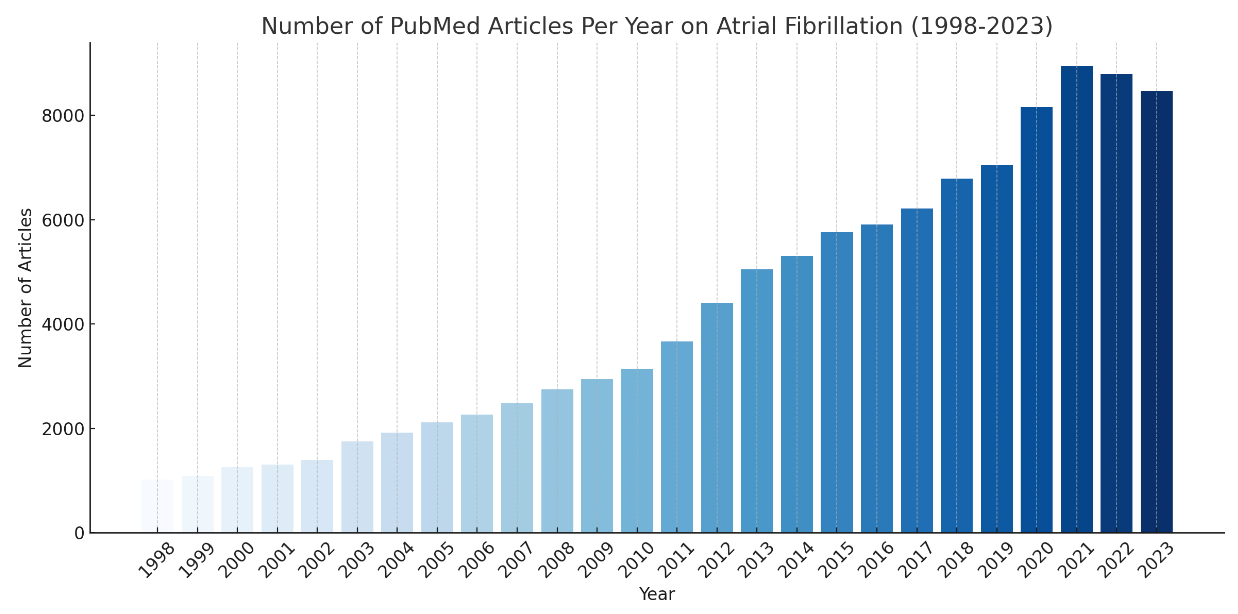
It has been 25 years since the seminal work from Michel Haïssaguerre showed where Atrial Fibrillation originates from in the heart. It has been cited by other Scientific papers more than 10,000 times. However, the progress in AF research in 2023 continued at an impressive pace. And importantly the quality of the trials continuea to push boundaries and innovate to improve the care for a growing number of individuals with the arrhythmia.
Many of the published trials in 2023 have been ground-breaking and set the foundation for real-world improvements in AF care in 2024. And so as the year comes to an end, I want to highlight three trials from this year that I predict will change the way we care for patients with AF in 2024.
The ADVENT trial- Pulsed field ablation is as good as traditional ablation
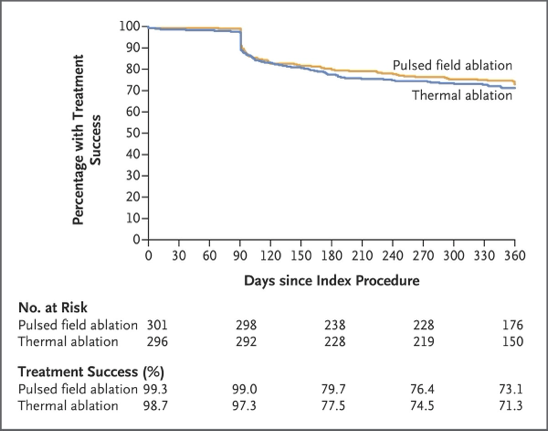
Key messages: This randomised controlled trial showed that catheter ablation using a new 'Pulsed Field' technology was no worse than traditional 'Radio-frequency' (heat-based) catheter ablation in patients with paroxysmal (intermittent) Atrial Fibrillation.
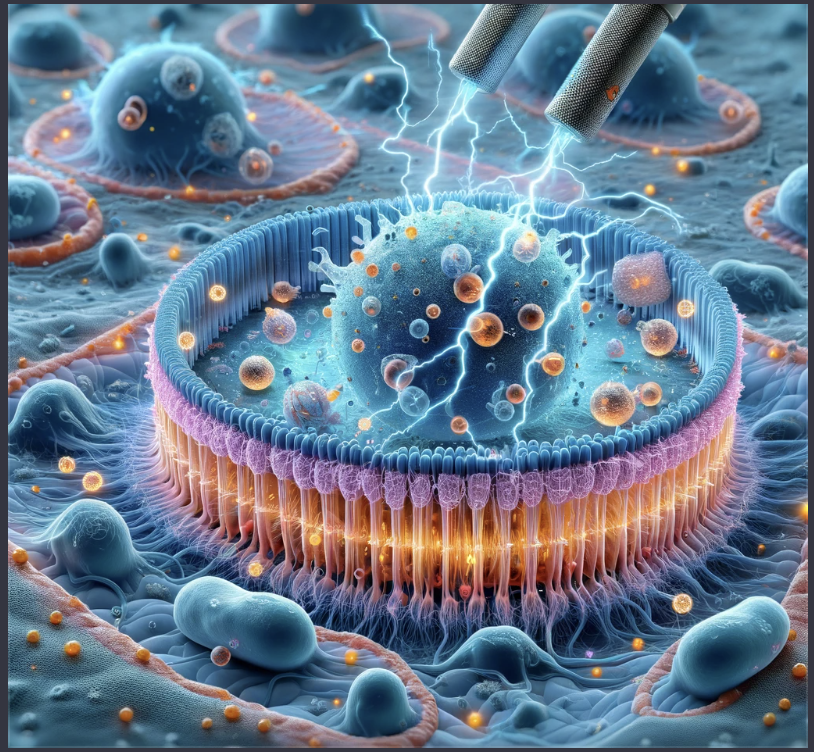
Why it is important: Pulsed Field ablation has been a hot topic presented and discussed at every AF-related conference I have been to in the last few years. It uses 'electroporation' technology to deliver high-frequency electrical pulses to selectively target heart cells and potentially mitigate the risk of damage to surrounding organs and structures.
After a lot of enthusiasm, the ADVENT trial was a randomised controlled study wherein the patients were blinded to the technology used on them as well. So it was a methodologically sound trial design to evaluate this relatively new technology against the clinical gold standard. The results were impressive in their equivalence- the freedom from AF was strikingly similar between the two patient groups, as was the safety profile (73.3% of patients were free of recurrence one year after Pulsed Field ablation vs 71.3% with RF ablation). The authors highlighted that the operators were familiar with traditional ablation and this was early use of Pulsed field ablation by 65 operators across 30 centres.
Impact on 2024: The ADVENT Trial was included in this list to represent the body of research in 2023 that has improved our appreciation of what Pulsed Field Ablation can (and can't) do. There were still rare complications and AF did recur in almost 30% of patients. It is unclear why these recurrences occurred or whether they were clinically significant- only one patient needed repeat ablation and only one needed amiodarone. We shall be acquiring this ablation technology in 2024 at our Institution so I will write a more detailed breakdown then.
The Semaglutide trials- GLP-1 drugs improve cardiovascular outcomes
Key messages: The SELECT trial was the original Randomised Controlled Trial in 2023 to show that 12-months of Semaglutide (otherwise known as Ozempic) led to an improvement in Cardiovascular outcomes (heart attack, death, stroke) in obese patients with cardiovascular disease with Diabetes. STEP-HFpEF then demonstrated these cardiovascular benefits in non-diabetic patients who were obese with cardiovascular disease. We discussed the impact of this trial on patients with AF in September.
Why it is important: By 2030- more than half the World's population will be obese if current trends continue. Not just limited to Western countries, but in India and China also. As BMI increases, the prevalence of AF increases. Weight loss improves AF burden, AF symptoms and ablation outcomes. Some Healthcare professionals may be uncomfortable with the medicalisation of obesity and using a drug to treat what is a lifestyle-mediated disease in many people. But the association with AF and cardiovascular disease is clear. Lifestyle changes certainly help but are not feasible for everyone. If Ozempic can improve AF outcomes, it may provide an additional therapeutic strategy.
Weight loss improves AF burden, AF symptoms and ablation outcomes.
Impact on 2024: A lot of big decisions are coming in 2024 in the Semaglutide space. We don't know what it will be licensed for or which patients will be able to access it. In the UK, Patients with diabetes and non-diabetics with a BMI >35kg/m2 are able to access it. There are no recommendations based on cardiovascular disease- because we don't have the trial data about how non-obese patients with cardiovascular disease patients will respond. So for AF, we will need a Randomised Controlled Trial, firstly in obese patients to evaluate whether Semaglutide can produce the health benefits seen with lifestyle-based weight loss. One of the other big challenges will be to know what we do after the 1-year course. The SURMOUNT-4 trial published just two weeks ago showed that discontinuation led to putting the weight back on. Do the cardiovascular risks return? We don't know yet. Many answers to come in 2024.
CASTLE-HTx- Catheter Ablation helps in end-stage heart failure
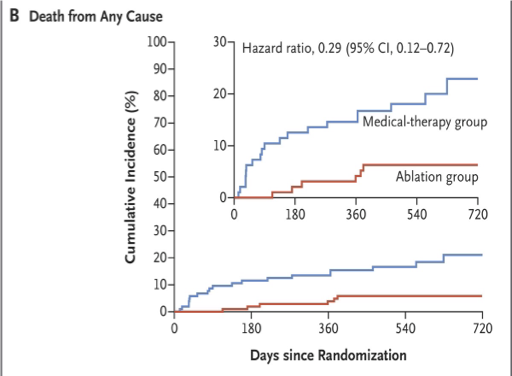
Key messages: This randomised trial out of Germany enrolled 194 patients with end-stage heart failure- patients who had been referred for consideration of heart transplantation. Half underwent catheter ablation and half continued on medical therapies only. The catheter ablation group had a lower risk of death or needing to progress to heart transplantation or LVAD (a mechanical heart pump in patients waiting for a transplant or were too sick for a transplant) within 18 months.
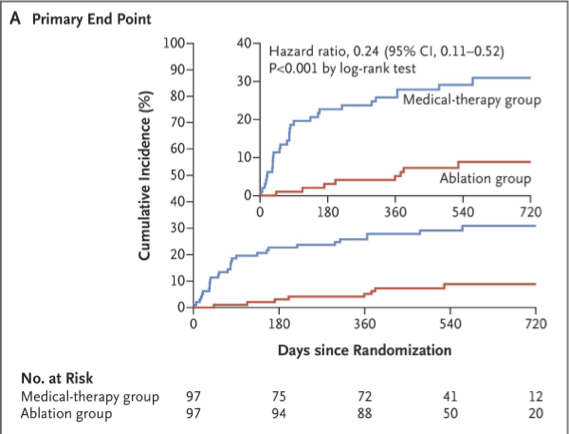
Why it is important: Firstly, the investigators should be commended for conducting a study on this incredibly sick and frail patient group. We know the risk of complications and procedural complexity are higher in these patients. In CASTLE-HF (the study we discussed last week) the patients with the most severe pump weakness benefitted the least. Thus, these patients are often excluded from typical Heart Failure trials. So it is great to finally have evidence about the outcomes of Catheter Ablation in these extreme cases.
It is hard to counsel patients on the best thing to do in the situation of AF and end-stage heart failure. On one hand, the ablation risk is higher and a complication could render them ineligible for Heart Transplantation. However it does seem like catheter ablation can help. it could have a meaningful effect on survival and help a patient avoid the substantial risks of transplantation or LVAD, especially when access to these options is so limited.
Impact on 2024: These are some of the sickest patients we manage in Cardiology. Although we have a range of tablets to help patients who develop Heart Failure, the outcome for patients with advanced heart failure who do not receive heart transplantation remains poor. Heart Failure severity should not be prohibitive to consideration of catheter ablation and paradoxically, the sicker the patient, the relative benefit in appropriately selected patients seems to be larger. So we should see more heart failure and end-stage heart failure patients in our AF clinics for consideration of catheter ablation.
Happy New Year to everyone reading and all the best for 2024!
Full papers to read:
ADVENT trial: Reddy, V. Y. et al. Pulsed Field or Conventional Thermal Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 389, 1660–1671 (2023).
SELECT trial: Lincoff, A. M. et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N. Engl. J. Med. 389, 2221–2232 (2023).
CASTLE-HTx trial: Sohns, C. et al. Catheter Ablation in End-Stage Heart Failure with Atrial Fibrillation. N. Engl. J. Med. (2023) doi:10.1056/nejmoa2306037.