AF ablation in special populations

How do we measure success?
Understanding the Variability in AF Ablation Outcomes
Atrial fibrillation (AF) ablation has been transformative in managing symptomatic AF- proving to be the most effective way to restore normal rhythm in this context. However, success rates vary significantly in selected patient populations, where factors such as AF type, structural heart changes, or additional comorbidities can lower the chances of positive outcomes. Paradoxically, these patients may also suffer more symptomatic and debilitating AF, leading to more urgent consideration of treating the arrhythmia. So the scenario then arises of higher risk (or perhaps a lower chance of benefit) vs higher reward. And if a patient is willing to accept a 50% success rate and understands the risks and benefits, should anyone have the right to prevent them from undergoing the procedure?
Recent NHS England guidance:
In December 2022, NHS England published this Clinical Commissioning policy recommending AF ablation for routine commissioning as a treatment option for paroxysmal and persistent atrial fibrillation within [outlined] criteria.
The document highlighted circumstances in which AF ablation they recommend AF should not be considered. Their exclusion criteria included the following:
Paroxysmal and Persistent AF:
Life expectancy ≤ 5 years.
Planned other cardiovascular interventions.
An absolute contraindication to anticoagulation therapy or heparin.
Significant and permanent liver failure.
Heart attack or stroke within 3 months prior to treatment.
Uncontrolled hypertension.
Persistent AF only:
Stage 4 heart failure symptoms.
Hypertrophic cardiomyopathy.
Duration of AF >2 years.
Significant mitral valve disease i.e. severe mitral stenosis or regurgitation or a mechanical mitral valve replacement.
There is a lot to consider in this document and we'll explore it further in a future post but for today, I am highlighting this paragraph to demonstrate that UK commissioning groups have highlighted patients that be excluded from catheter ablation due to limited effectiveness. So let's take one step further back- how do you determine effectiveness to identify groups of patients for whom ablation is 'ineffective'?
Traditional measures of AF ablation success
Research studies are the early paradigm wherein ablation outcomes are evaluated. To be able to measure the impact and compare it against other treatment options, an objective, undisputable outcome allows for easier delineation- like how yes/no answers are easier to interpret than '1 to 10 Likert scales' or free text-written answers.
Ablation success is conventionally measured by the absence of any AF recurrence, with some studies defining positive events as any lasting more than 30 seconds. Sometimes time-to-event analysis is also performed to reflect how long patients stay free of AF as well. This approach is simple and objective but may not reflect what is truly important to patients.
Alternative metrics can include the use of continuous monitoring devices such as implantable cardiac monitors to give a percentage AF burden or considering the subjective impact on patients using questionnaires.
Hypertrophic Cardiomyopathy and AF Ablation
We have been exploring the use of these alternative metrics in one of the aforementioned special populations- patients with hypertrophic cardiomyopathy. And recently, we presented our findings from our registry at Barts Hospital at the EHRA (European Heart Rhythm Association) conference in April 2023.
What is hypertrophic cardiomyopathy?
Commonly abbreviated to HCM, hypertrophic cardiomyopathy is the most common inherited cardiac condition affecting 1 in 500 people. It is a disease of the heart muscle that can cause it to become stiff and thickened- preventing proper pumping. This can lead to heart-related symptoms and can also increase the risk of sudden death. You can find out more about the condition on the BHF website. These patients are also at an increased risk of AF and due to the stiffness of the heart and structural abnormalities can be more vulnerable to symptoms from the AF when it comes on. Using the traditional measures of ablation success, the outcomes are lower than in the general population.
What we did
We identified patients with HCM and AF who underwent AF ablation procedures at Barts Hospital. We then sub-selected patients who already had a cardiac device previously implanted for other reasons (for example a pacemaker, a defibrillation or an implantable monitor) so that we could precisely measure the percentage AF burden before and after the ablation and confidently say we hadn't missed any events. We then monitored the patients for an average of >2.5 years.
Our results- lots of charts!
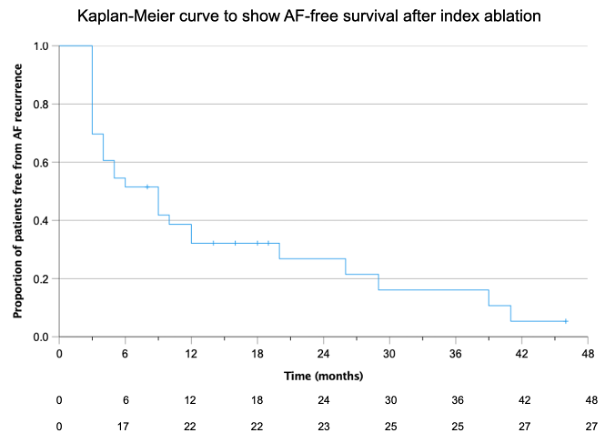
- If we use traditional measures, ablation appears to be ineffective After the first ablation, AF recurred in 27 (82%) patients with a median time to first AF recurrence of 8 (3-17) months.
.
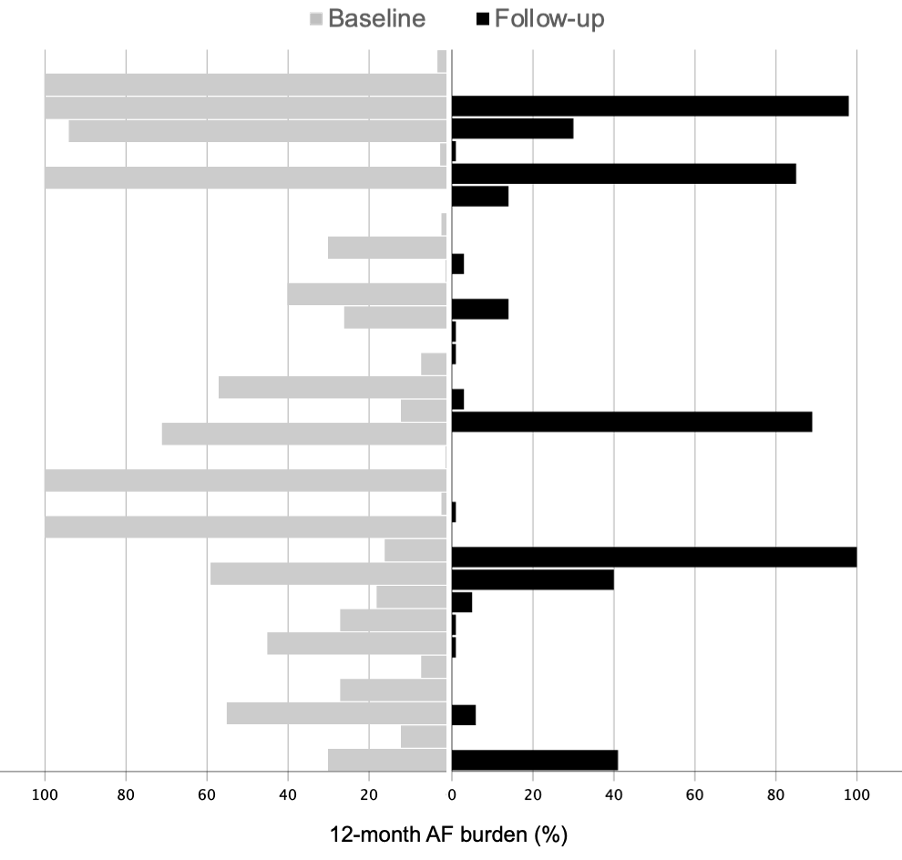
2. But looking at % AF burden, there is a significant decrease after ablation. Before ablation, patients were in AF for a median of 27% of the time (three-quarters had an AF burden between 7-59% ). After ablation(s) this burden significantly reduced to a median of 0% (three-quarters had 0-30%).
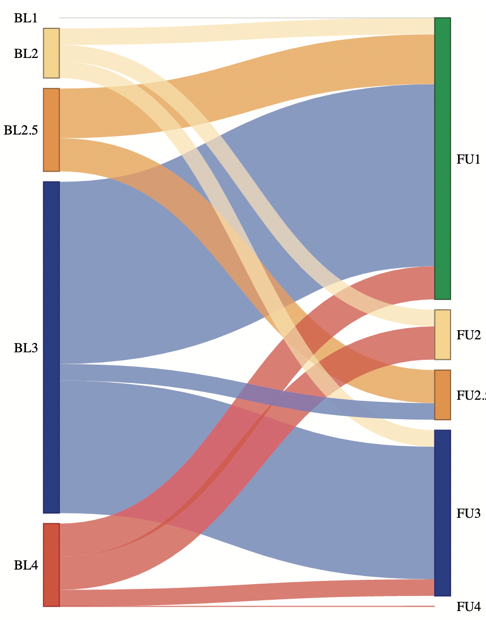
3. And patients reported a better quality of life too. 20 (61%) patients reported an improvement by at least 1 EHRA class (a standardised measure of the impact of AF on patient activities). 20 (61%) of patients also reported no troublesome symptoms or no symptoms at all after their ablation(s)- this includes 11 patients who had an AF recurrence i.e. by traditional measures would have been deemed a failure.
What does this mean?
Although the trends in this study are clear, we have to recognise it is quite a small sample. The patients studied were selected by their clinician for AF ablation and so may have not represent 'all' patients with HCM, especially as the group studied had pre-existing cardiac devices for other reasons too. Also, this is 'observational' data i.e. there may well be other contributing factors that led to the improvement in quality of life and AF burden.
However, the results are promising and have implications for patients without HCM as well. We believe we have shown that you can measure AF burden and quality of life as alternative measures in patients undergoing ablation. AF ablation is done to reduce symptoms and improve quality of life. So let's measure what matters. We should measure the impact on quality of life and arguably that should contribute to commissioning decisions. We don't have enough information yet on these metrics and that's probably why traditional measures still have to be relied on. Using 'PROMs' (questionnaires about patients' quality of life) was one of the other recommendations from the NHS England policy so hopefully that will help generate additional data based on these alternative metrics. We are completing a multi-centre, international review of these metrics in patients with HCM that will (hopefully) be published later this year.